Supportive Care
The goal of supportive care is to improve symptoms and complications of anemia in MDS
Supportive therapies may be used alone or in combination and generally consist of transfusions and growth factors. Supportive care should also include nonpharmacologic approaches such as psychosocial support and quality of life assessment. Some patients may only require observation and monitoring.Treating Myelodysplastic Syndromes. November 21, 2024. American Cancer Society. Accessed May 21, 2025. https://www.cancer.org/content/dam/CRC/PDF/Public/8746.00.pdf Platzbecker U et al. Leukemia. 2021;35:2182-2198. Platzbecker U. Blood. 2019;133(10):1096-1107. Mastanzade M. Hematol Transfus Cell Ther. 2024;46(S7):S1-S20.

While supportive care can be a beneficial clinical approach to identify the appropriate time to initiate active treatment or symptom management, it is generally not a long-term solution, and further treatment is often needed.Treating Myelodysplastic Syndromes. November 21, 2024. American Cancer Society. Accessed May 21, 2025. https://www.cancer.org/content/dam/CRC/PDF/Public/8746.00.pdf Platzbecker U et al. Leukemia. 2021;35:2182-2198. Platzbecker U. Blood. 2019;133(10):1096-1107. Mastanzade M. Hematol Transfus Cell Ther. 2024;46(S7):S1-S20.
Transfusions and chelating agents
Red blood cell (RBC) transfusions are an important part of supportive care for patients with symptomatic anemia. However, many patients become dependent on RBC transfusions, which has been associated with iron overload (if unmanaged), increased risk of death, increased risk of progression from MDS to AML, and poor quality of life.Germing U et al. Hemasphere. 2019;3(6):e314. Platzbecker U et al. Leuk Res. 2012;36:525-536. Soper J et al. Patient Relat Outcome Meas. 2022;13:31-38. Lemos MB et al. Eur J Haematol. 2021;107:3–23.

~40%
of patients with MDS who develop anemia become transfusion dependent.Zeidan AM. Blood Rev. 2013;27:243-259.

Transfusion dependence is associated with a worse prognosis and a
44%
increased risk of deathLemos MB et al. Eur J Haematol. 2021;107:3–23.
Benefits and drawbacks of RBC transfusions include:Germing U et al. Hemasphere. 2019;3(6):e314. Supportive Care. Leukemia and Lymphoma Society. Accessed May 21, 2025. https://www.lls.org/myelodysplastic-syndromes/treatment/supportive-care
 Improved blood cell counts and correction of anemia
Improved blood cell counts and correction of anemia- Immediate relief from anemia-related symptoms, such as shortness of breath and fatigue
 Adverse effects, such as iron toxicity and RBC alloimmunization
Adverse effects, such as iron toxicity and RBC alloimmunization
Frequent transfusions may also cause significant clinical complicationsOliva EN et al. Blood Rev. 2021;50:100851. Balducci L. Cancer. 2006;106:2087-2094.
To learn more, view the tabs below. Each tab contains helpful information.
Transfused patients with MDS have a greater incidence of comorbid conditions compared with non-transfused patientsGoldberg SL et al. J Clin Oncol. 2010;28:2847-2852.

Reproduced with permission from J Clin Oncol.Goldberg SL et al. J Clin Oncol. 2010;28:2847-2852.
Data based on a retrospective review of US Medicare claims of beneficiaries aged ≥ 65 years in 2003 with a 3-year follow-up. A limitation of this study lies in the use of claims data, which are less detailed and have less accurate clinical information. These types of data may also be at risk for over- and/or under-reporting due to coding and naming discrepancies.Goldberg SL et al. J Clin Oncol. 2010;28:2847-2852.
- Among patients receiving transfusions, 82.4% were diagnosed with a cardiac event compared with 67.1% who did not receive transfusions. Diabetes, dyspnea, hepatic disease, and infectious diseases also had a higher prevalence in patients with MDS receiving transfusions during the 3-year follow-up.Goldberg SL et al. J Clin Oncol. 2010;28:2847-2852.
Alloimmunization is an immune response against foreign RBC antigens that causes hemolytic reactions, which can make finding compatible blood for future transfusions more difficultThein SL et al. Haematologica. 2020;105:539-544. Molina-Aguilar R et al. Transfus Med Hemother. 2020;47:152-159.
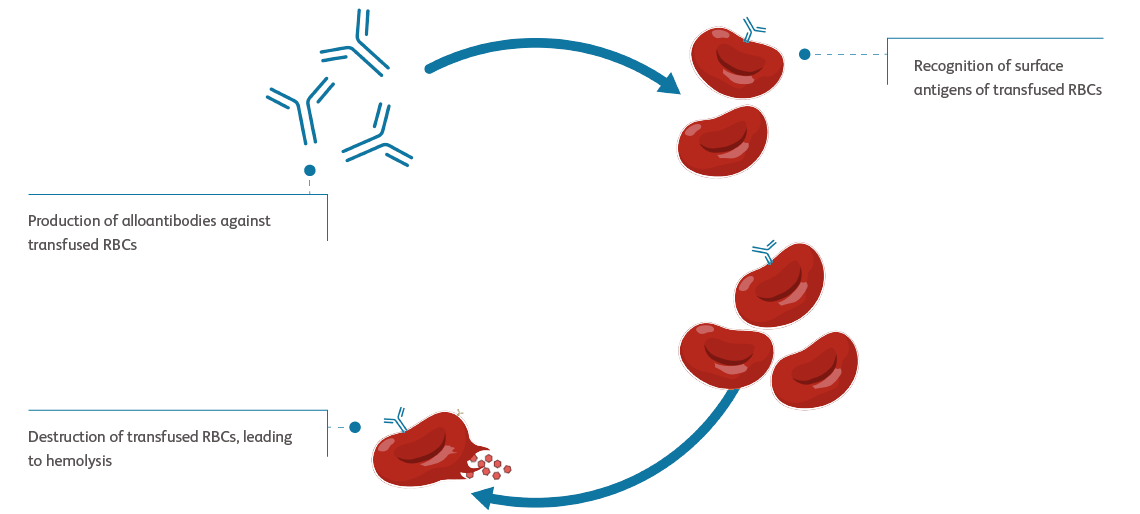
Adapted from Haematologica.Thein SL et al. Haematologica. 2020;105:539-544.
RBC, red blood cell.
- The risk of alloimmunization increases with an increasing number of RBC transfusionsZalpuri S et al. BMJ Open. 2012;2:e001150.
Chronic transfusion may also lead to iron accumulationWeber S et al. Front Immunol. 2020;11:627662.
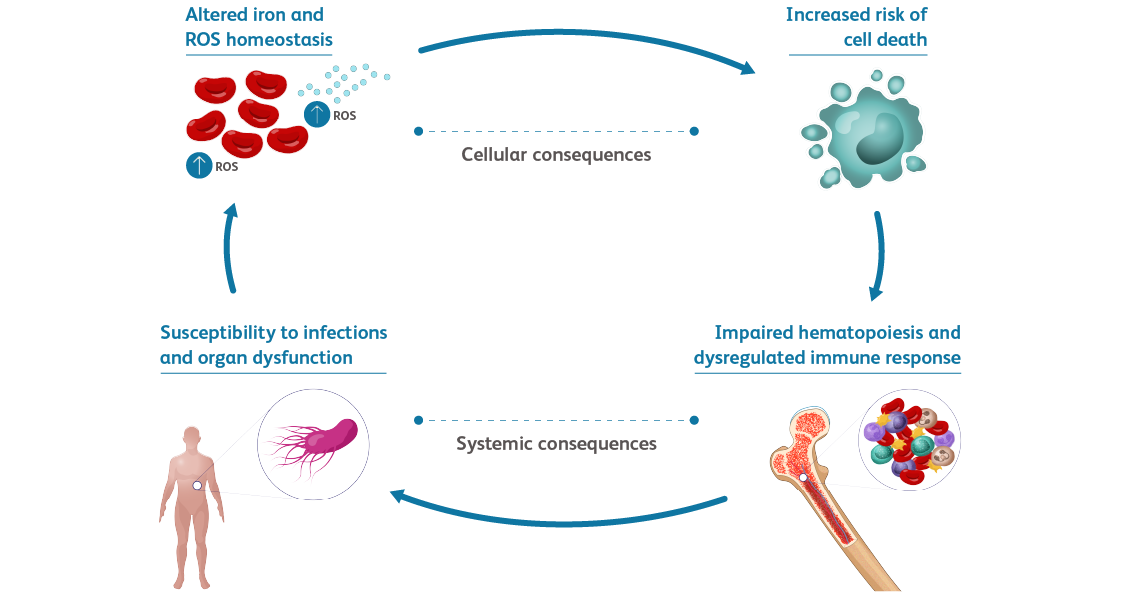
Adapted from Front Immunol.Weber S et al. Front Immunol. 2020;11:627662.
ROS, reactive oxygen species.
- Excess iron can be toxic to several organs and can cause tissue damageWeber S et al. Front Immunol. 2020;11:627662.
- It can also affect components of the immune system and increase the risk of infectionsWeber S et al. Front Immunol. 2020;11:627662.
Iron chelation therapy
.png)
Iron overload can lead to altered iron and reactive oxygen species homeostasis, leading to increased risk of cell death and dysregulated immune response, thereby increasing susceptibility to infections and organ dysfunction.Treating Myelodysplastic Syndromes. November 21, 2024. American Cancer Society. Accessed May 21, 2025. https://www.cancer.org/content/dam/CRC/PDF/Public/8746.00.pdf

Excess iron may accumulate in the liver, heart, and other vital organs, usually only occurring in patients receiving multiple transfusions over a period of years.Platzbecker U et al. Leukemia. 2021;35:2182-2198.
.png)
Chelating agents bind to excess iron and remove it from the body to mitigate the risk and toxic effects of iron overload.Platzbecker U. Blood. 2019;133(10):1096-1107.

Adverse effects due to chelating agents include injection-site reactions and gastrointestinal disturbances. Rare but severe events such as renal failure have also been reported.Mastanzade M. Hematol Transfus Cell Ther. 2024;46(S7):S1-S20.
Growth factors
Granulocyte colony-stimulating factor (G-CSF) is often used to help increase white blood cell (WBC) production to treat frequent infections due to neutropenia. For MDS-associated anemia, G-CSF may be combined with an ESA to promote synergistic enhancement of the erythroid response.

In patients with MDS-associated anemia, G-CSF is:Treating Myelodysplastic Syndromes. November 21, 2024. American Cancer Society. Accessed May 21, 2025. https://www.cancer.org/content/dam/CRC/PDF/Public/8746.00.pdf Platzbecker U et al. Leukemia. 2021;35:2182-2198. Platzbecker U. Blood. 2019;133(10):1096-1107.
- Not routinely used for infection prophylaxis
- Typically administered subcutaneously or intravenously
- Used in cases of frequent infection or low WBC counts
Benefits and drawbacks of G-CSF include:Platzbecker U. Blood. 2019;133(10):1096-1107. Germing U et al. Hemasphere. 2019;3(6):e314.
- Possible improvement in the likelihood of erythroid response in combination with an ESA
- Reduction in neutropenia
- Adverse effects, such as bone pain, thrombocytopenia, and leukocytosis
Nonpharmacologic supportive care
In addition to pharmacologic treatments for anemia, such as RBC transfusions and growth factors, supportive care regimens should also involve clinical monitoring and observation, psychosocial support, and quality of life assessment.Platzbecker U et al. Leuk Res. 2012;36:525-536. Soper J et al. Patient Relat Outcome Meas. 2022;13:31-38.

Figure ReferencesPlatzbecker U et al. Leuk Res. 2012;36:525-536. Soper J et al. Patient Relat Outcome Meas. 2022;13:31-38. Lemos MB et al. Eur J Haematol. 2021;107:3–23.
Learn more

